
Prognosis of a Polished Surface Basal Implant
Dr. Irfan Ali Motiwala* – MDS Oral and maxillofacial surgery, Dr. Motiwala Dental clinic and Implant center, Hyderabad, Telangana, India *Corresponding Author
Dr. Tejaswi Bathina – MDS, Oral Medicine, and Radiology, Dr. Motiwala Dental clinic and Implant center, Hyderabad, Telangana, India
Dr. Suhela Motiwala – BDS, Dr. Motiwala Dental Clinic and Implant Center, Hyderabad, Telangana, India
Available Online at: www.worldwidejournals.com
Abstract
The importance of detecting anatomical variations plays an important role in avoiding certain inadvertent complications, minor/major. The occurrence of multiple mental foramina is not uncommon but is unusual. It is very important to recognise these anatomical alterations while performing surgical interventions, or anesthetising the mental nerve, especially while placing implants in this region. Unintended damage to the foramen and its contents, during these procedures, might cause sensory disturbances for the patient. In this case series of two patients, we are presenting the identification anatomical variation of mental foramen where two mental foramina were identified unilaterally in both patients.
Keywords
Mental foramen, accessory foramen, CBCT, anatomical variations
Introduction
A thorough clinical and radiological evaluation, before executing surgical procedures is important for avoiding any unintended consequences during or after surgeries. Dental implant surgery is one of the most common treatments rendered to patients with missing teeth. Analysing the exact location of anatomical and/or vital structures helps in avoiding nerve injury besides some other minor complications1. Inferior alveolar nerve block is used to anesthetise the mandible during any surgical treatments in the lower jaw. The inferior alveolar nerve, continues as mental nerve after emerging through the mental foramen and innervates the anterior teeth, lip and chin region of the mandible2,3.
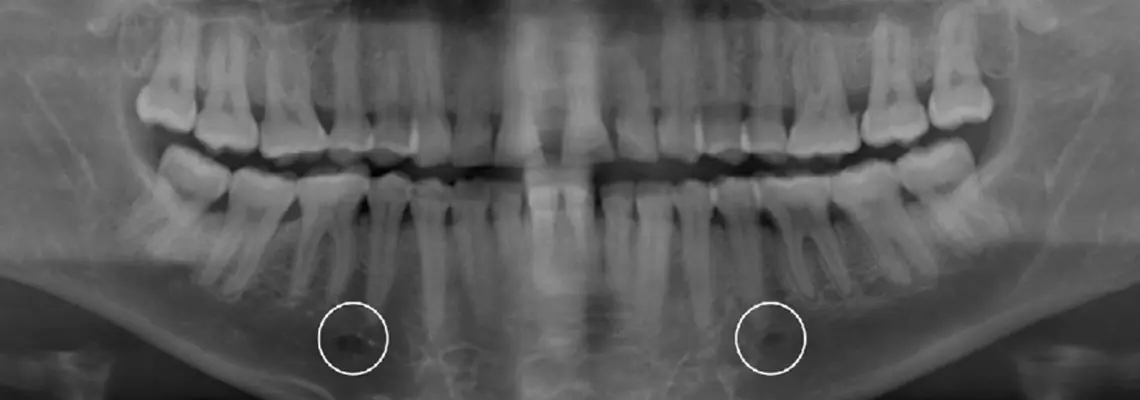
Mental foramen is a round/oval-shaped opening usually located below the first and second premolars, or in some instances, below the first molar. Mental and/or incisive nerve block is administered taking this point as a reference2. Although the position of mental foramen can be seen on an orthopantamograph (OPG), its exact location can only be visualized with a multiplanar radiographic image. This evaluation will not only help in rendering an effective mental nerve block, when administered but also prevents unintended injury to the canal and its content4.
There have been several studies carried out in identifying the normal aspects of mental foramen as well as its anatomical variations. In this case series of two patients, we are mentioning an unusual occurrence of two mental foramens observed unilaterally when planning implant surgery.
Case Report 1:
A 56-year-old male patient came to the clinic with a complaint of missing teeth and loosening of his teeth region since four to five years. he gave a history of several missing teeth, and gaps between his bridges that has compromised his diet and esthetics. On clinical examination, there were several missing teeth and generalised periodontitis with mobility in relation to most of the teeth intact. All the teeth evaluated showed that the prognosis of saving these teeth was very bad and so the patient was advised to undergo extractions followed by rehabilitation with dental implants.
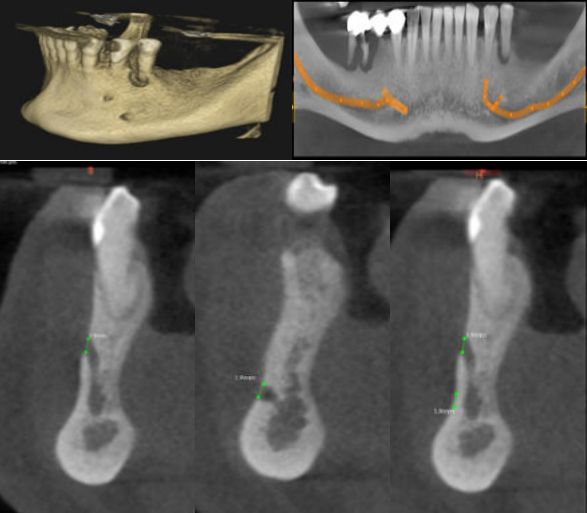
The patient was informed about the entire procedure and a surgery was planned after prescribing some antibiotics. Before the procedure, a full mouth orthopantamograph (OPG), and a three-dimensional (Cone Beam computed tomography) CBCT scan was taken to check for vital structures. The scan showed otherwise normal findings, but for the presence of two mental foramen on the left side. The foramen were oval in shape and present in between the two premolars, placed one above the other. One foramen was distanced at 18.8mm from the inferior border of the mandible and the other foramen, at a distance of 10.1mm. The right side of the mandible however showed a single oval-shaped foramen, distanced at 12.5mm from the inferior border of the mandible.
Case Report 2:
A 24-year-old male patient, came to the clinic with a complaint of missing teeth in his upper and lower, front and back teeth region since 7 years. His history revealed that the patient has lost his deciduous teeth but were not replaced by permanent teeth. His medical history revealed that the patient was diagnosed with a congenital disorder of ectodermal dysplasia. He was affected with disturbances in the formation of his teeth along with the presence of pigeon chest (pectus excavatum), which was corrected by surgery one year ago. On clinical examination, there were missing teeth in relation to his upper anterior, and premolar teeth and lower posterior teeth. Overly retained deciduous teeth were noted in the lower anterior segment of his dentition. There was ectopic eruption of upper left canine, which was positioned in a much posterior region than its normal position.
A full mouth orthopantomographic image was taken to evaluate the eruption of permanent teeth. The OPG showed several overly retained deciduous teeth, missing teeth, and no permanent teeth/tooth buds for the missing teeth. This led to a diagnosis of partial anodontia and the patient was described about the treatment options available for restoring his teeth. The patient wanted to get missing teeth replacement with the aid of dental implants and therefore was scheduled for surgical intervention.
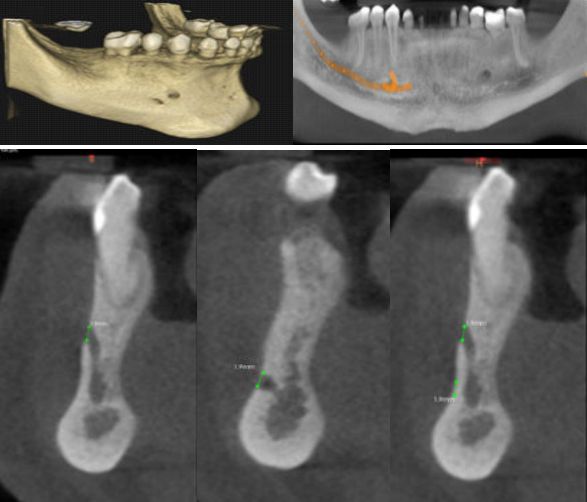
Before the procedure, a three-dimensional CBCT scan was taken to evaluate the location of vital structures. On the right side of his mandible, two mental foramina were noted. One was found on the distal aspect, below the apex of first premolar and the other foramen was noted a little anterior to it. The foramen were present at a distance of 11.3mm and 14.8mm from the inferior borer of the mandible. The left side was normal with a single foramen noted below the apex of the second premolar.
Discussion
The occurrence of anatomical variations when analysing the soft and hard tissue findings is usually neglected. These variations, when identified before performing any surgical interventions would help in avoiding few minor/ major complications. The inferior alveolar nerve and mental nerve are the vital structures in the mandible, whose thorough 5,6 analysis helps in arriving at a favourable surgery in the mandible. The mental foramen is generally a single, bilateral opening found near the apex of the second premolar. There are, however, few anatomical variations in regard to their size, number, and location. Multiple mental foramens have been identified either unilaterally or bilaterally in around 0.2% to 10.6%. Previous studies also show the presence of 7,8 three mental foramens.
The diameter of mental foramen ranges from 1.8mm to 5.1mm with a mean diameter of 3mm. the diameter of accessory mental foramen are generally less than 1mm implying that they do not pose much of a risk, 3, 8, 9 otherwise. In the present case series, the diameters of mental foramen and accessory foramens were found to be 2.6mm and 1.1mm in one patient, and 1.9 and 1.9mm in another patient. Although one patient showed a relatively smaller accessory foramen of 1.1mm diameter, the other patient had both the foramens of the same diameter.
Considering the location of the foramen, around 50% of the population has mental foramen below the apex of the second premolar. 20-25% have it anterior to the second molar, i.e., in between the first and second premolar. 24% was found to be placed posterior to the second premolar, near the first 3,8,10 molar and the remaining 1%, anterior to the first premolar. Our report shows the presence of foramens: one below the second premolar and the other in between the first and second premolars. The accessory foramen is usually positioned posterior and inferior to the main foramen. When the accessory canals are placed inferiorly, there is minimal to no risk of nerve impingement as the treatment plan would be made taking the superior canal as a reference. Also, the diameter of the accessory canal is usually less, which is below 1mm. So, no great risk is implicated in such conditions. But in cases where the diameter is more than or equal to the main foramen, caution must be taken while making a treatment plan so that the nerve is not impinged.
Conclusion
When multiple mental foramina are present, the accessory foramens are usually smaller in diameter and are placed below the primary foramen. These instances generally do not pose much problem, as they are below the primary foramen. But care must be taken in conditions where the diameter of the accessory foramen is similar to that of the primary foramen or where the position of the foramen might affect the treatment procedure. So that necessary precautions are taken to avoid any unintended complications during minor or major surgical interventions carried out in this area.
References
1) Misch, Kelly DDS*; Wang, Hom-Lay DDS, MSD, PhD†. Implant Surgery Complications: Etiology and Treatment. Implant Dentistry: June 2008 – Volume 17, Issue 2, P 159-168
2) Iwanaga J, et al. Accessory mental foramina and nerves: application to periodontal, periapical, and implant surgery. Clin Anat. 2016;29(4):493–501.
3) Zmysłowska-Polakowska, E., Radwański, M., Łęski, M. et al. The assessment of accessory mental foramen in a selected polish population: a CBCT study. BMC Med Imaging 17, 17 (2017).
4) Iwanaga, Joe; Saga, Tsuyoshi; Tabira, Yoko; Nakamura, Moriyoshi; Kitashima, Sadaharu; Watanabe, Koichi; Kusukawa, Jingo; Yamaki, Koh-Ichi (2015). The clinical anatomy of accessory mental nerves and foramina. Clinical Anatomy, 28(7), 848–856.
5) Greenstein, Gary; Tarnow, Dennis (2006). The Mental Foramen and Nerve: Clinical and Anatomical Factors Related to Dental Implant Placement: A Literature Review. Journal of Periodontology, 77(12), 1933–1943.
6) Shan, S., Zhong, S., Li, J. et al. Systematic review and meta-analysis of mandibular canal variations on cone beam computed tomography. Oral Radiol 38, 445–451 (2022). https://doi.org/10.1007/s11282-022-00610-5
7) Ramadhan, Anwar & Messo, Elias & Hirsch, Jan. (2010). Anatomical variation of mental foramen. A case report. Stomatologija / issued by public institution “Odontologijos studija” … [et al.]. 12. 93-6.
8) Hearty Deepak J J, Nelson A, Bharathi C S, Deepthi D A. Triple mental foramina: CBCT Findings of an unusual anatomical variant. J Indian Acad Oral Med Radiol 2018;30:423-6
9) Shalash, M., Khallaf, M.E. & Ali, A.R. Position and dimensions of the mental foramen and presence of the anterior loop in the Egyptian population: a retrospective CBCT study. Bull Natl Res Cent 44, 110 (2020).
10) Bello SA, Adeoye JA, Ighile N, Ikimi NU. Mental Foramen Size, Position and Symmetry in a Multi-Ethnic, Urban Black Population: Radiographic Evidence. J Oral Maxillofac Res. 2018 Dec 30;9(4): e2.






